Abstract Good health is an invaluable asset for better economic productivity, both at the individual and at the national level, but above all it is valued by those who own it as a pre requisite for better quality of life and better standard of living. The biological differences and the life process of women necessitate special attention for ensuring better health for women. Beginning of Menstrual Cycle, Pregnancy, lactating period and menopause are the milestones in the life of ordinary women as there will be lot of physio- psychological changes. Each period requires special care in terms of dietary practices, physical exercises, rest and social interactions. Towards achieving this goal the United Nations, Government of India and the Government of Karnataka have made several efforts. The present paper has been prepared using the NFHS- IV data to understand the status of health of women in Karnataka. The presence of anemia both among pregnant (39.6% in urban and 48.7% in urban areas) and non pregnant women (43.0% in urban and 46.2% in urban areas), obesity, low body mass index and the domestic violence (20%) indicates the need for an integrated approach for the health of women. This calls for a shift from reproductive health approach to life cycle approach for promoting the health of women. Keywords: reproductive approach, health problems of women, life cycle approach. Health Status of Women in Karnataka: An analysis Good health is an invaluable asset for better economic productivity, both at the individual and at the national level, but above all it is valued by those who own it as a pre requisite for better quality of life and better standard of living. Health does not include only physical health. The World Health Organization defines health as a state of complete physical, mental and social well being and not merely the absence of disease or infirmity. Gender is also one of the main factors that influence on the health of the individuals. Inequality between men and women is one of the most critical disparities in the developing nations in general and India in particular. Apart from the existing the inequality, the biological differences and the life process of women necessitates special attention for ensuring better health for women. Beginning of menstrual cycle, pregnancy, lactating period and menopause are the milestones in the life of ordinary women as there will be lot of physio- psychological changes. Each period requires special care in terms of dietary practices, physical exercises, rest and social interactions. Rationale: The health of women is important as it not only affect the health of her own but also of the next generation. The importance of female health precedes and extends beyond the reproductive years to optimize completion of adolescent growth and establish body nutrient reserves before pregnancy and to maintain adequate nutritional status, particularly skeletal health, through the postmenopausal years. Efforts at International Level for promoting the health of Women: The Beijing Platform for Action reiterates the agreements reached at the 1994 International Conference on Population and Development (ICPD), in particular with regard to women’s reproductive health and rights, and added new commitments addressing the right of women to have control over and decide freely and responsibly on matters related to their sexuality, including sexual and reproductive health, free of coercion, discrimination and violence. Taking a holistic and life-cycle approach to women’s health, the Beijing Platform for Action proposed actions toward five strategic objectives. The first objective being Increase women’s access throughout the life cycle to appropriate, affordable and quality health care, information and related services. The Millennium Development Goals (MDGs) adopted in 2000 address women’s health in two of the eight goals. MDGs focuses on improving maternal health by reducing by three quarters, between 1990 and 2015.The Sustainable Goals adopted by the member nations of UN during September 2015 again calls for promoting health and well being and achieving gender equality. Methodology: The present paper is attempted to examine the indicators of health status of women in Karnataka using the NFHS 2015-16 data for analysis. The indicators chosen for analysis are status of Anemia, Obesity and Body Mass Index. Along with that the data on spousal violence has been used as it affects the health of women. Data from NFHS-4 covering 26,291 eligible women 15-49 years of age in Karnataka was being used to collect information on various health indicators of women. The aim of the paper is to identify the gaps and to come out with the suitable approaches towards the health of women across life span. National and Regional Response for the Cause: The National Health Policy of the Government of India has made special provisions for the health of women throughout her life cycle. In response to the national health policy the Government of Karnataka has been implementing several health promotional programmes through the health centers and the Department of women and child welfare. The programmes aiming at, provision of adequate nutrition for pregnant women, 100% institutionalization of deliveries, maternal health and safety have been implemented with the co ordination of both the health centers and department of women and child development. Institutional births have been increased in rural areas from 2005 – 06 family survey (64.7%) to the present survey 2015-16(95.4%). But the survey results shows the gap in many areas which will be discussed below. Another land mark is the enactment of PROTECTION OF WOMEN FROM DOMESTIC VIOLENCE ACT, 2005. The Deputy Directors of Women and Child Development Department and Child Development Project Officers of Integrated Child Development Projects have been appointed as Protection Officers by the Government. For effective implementation of the Act, Co-ordination Committees have been formed at State, District and Taluk levels. Special Treatment Units for women and children have been set up to provide facilities of counselling, medical aid, police assistance, legal assistance under one roof, to women who are victims of various atrocities. These units have been setup in all district hospitals, which function 24x7. These units are also provided with Toll free women helplilne 181. However the enactment of legislation and implementation has not brought much change in the violence status which remains to be 20% on an average during 2005-06 survey and 2015-16 survey. Contradictorily the spousal violence against pregnant women has been increased from 6.5% in 2005-06 survey to, 8.7% in 2015-16 survey. 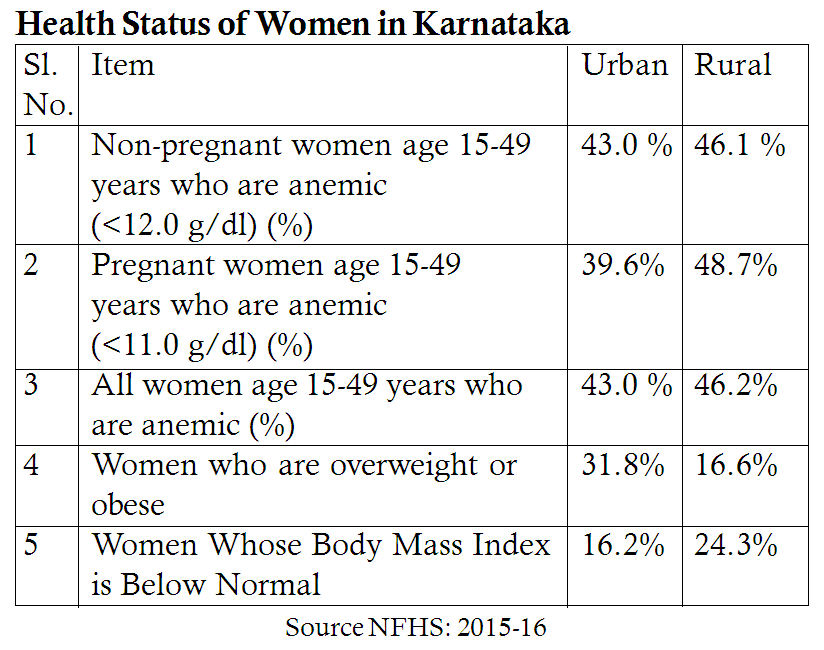 From the table it is understood that 43.0% of rural women and 46.1% of urban women are anemic. Another area of concern again is 39.6% of urban pregnant women and 48.7% of rural pregnant women are anemic which is a still more grave problem as it will not affect the women alone but also the offspring contributing for adding underdeveloped child. In urban areas, nearly 31.8% are obese and in rural areas 16.6% are obese. This has to be taken care as it affects the future course of the life of women. Urban women (16.2%) and Rural woman (24.3%) have body mass index below the normal level. The existing gap within the health status of women call for a life cycle approach to meet the health requirements of women. 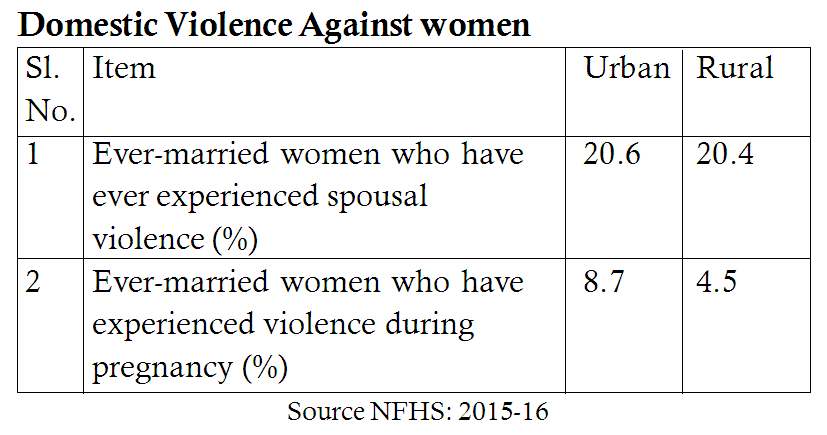 Even after a decade of the enactment of Domestic Violence (Prohibition) Act the women who have experienced spousal violence is 20% on an average both in the urban and rural areas. Another important area is women experiencing violence during pregnancy is comparatively more in urban areas at 8.7% and 4.5% in rural areas. Matter of concern as the cost of violence is much both on the individual and family.
Existing Gaps: 43.0% of women in urban areas and 46.1% women in rural areas are anemic. Anemia in the long run can affect the lives in different ways throughout the life cycle. For example during pregnancy it affects mother and child, during middle adulthood it affects the productivity and cognitive ability totally resulting in poor quality of life. Obesity, another problem affecting nearly 30% of urban women and 16% rural women is a matter of concern. Women who are overweight or obese are at increased risk of many cancers, including breast cancer and cancers of the reproductive system such as endometrial cancer. (Whitlock et all 2009) In spite of legislation and implementation of domestic violence prohibition programmes, the spousal violence against women has reduced since a decade and the violence against pregnant women is at rise, an alarming statistics about which the policy makers and the programme implementers need to think about. Suggested Approach to Address the Issue: This calls for a life course perspective on women’s health and understanding the link between past reproductive experiences and current or future health. Life course perspective highlights the potential for early intervention to reduce disease risk or severity. It also has intuitive relevance to women’s health needs (Rich Edwards, 2002) unlike sporadic disease episodes, reproductive and sexual health are relevant to almost all women and unfold across the life course, triggering healthcare needs in a more predictable fashion. A life course view of women’s health offers a more unified and woman-centered approach to health promotion, disease prevention and management, with implications for long-term, cross-generational health gain. (Barker M 2011). Furthermore, the physiological demands of pregnancy can act as an early ‘stress test’ that reveals risk of future chronic disease (Sattar and Greer, 2002) For example, although complications such as gestational diabetes resolve after delivery, they are associated with higher cardiovascular mortality in later life. Strategies to Address the Issue:
Conclusion: The attention to women’s health through out the life cycle and not only during pregnancy, childbirth and lactation will have long term benefits to the health of women as well society. This approach will bring significant improvement in over all health, productivity and improved quality of life of women which definitely includes maternal and child health. Improved health of women does contribute for social development. References:
Dr. R. Shivappa Associate Professor and Head, DOS in Social Work, University of Mysore, Mysuru Ms. Susmitha.B Assistant Professor, Postgraduate Department of Social Work, JSS College of Arts, Commerce and Science, Ooty Road, Mysuru, Karnataka |
Categories
All

Social Work Learning Academy
50,000 HR PROFESSIONALS ARE CONNECTED THROUGH OUR NIRATHANKA HR GROUPS.
YOU CAN ALSO JOIN AND PARTICIPATE IN OUR GROUP DISCUSSIONS. 
MHR LEARNING ACADEMYGet it on Google Play store
|


 RSS Feed
RSS Feed
SITE MAP
SiteTRAININGJOB |
HR SERVICESOTHER SERVICESnIRATHANKA CITIZENS CONNECT |
NIRATHANKAPOSHOUR OTHER WEBSITESSubscribe |
MHR LEARNING ACADEMY




50,000 HR AND SOCIAL WORK PROFESSIONALS ARE CONNECTED THROUGH OUR NIRATHANKA HR GROUPS.
YOU CAN ALSO JOIN AND PARTICIPATE IN OUR GROUP DISCUSSIONS.
YOU CAN ALSO JOIN AND PARTICIPATE IN OUR GROUP DISCUSSIONS.


|
|