 Abstract Introduction: Alcohol is the commonest substance abused by the human beings. The consumption of alcohol has been growing rapidly over the last two decades and alcoholic beverages are a standard lubricant at social gathering and those who refuse to consume run the risk of being social outcasts. Deaddiction and rehabilitation of alcoholics is a very crucial step to mainstream such demarginalised members of the society. The family and community at large play a very important role in reintegrating those with alcohol abuse. The community based camps provides easy access for those addicted to overcome their illness in a reassuring environment. With this background, the present study was conducted with the objective to assess the Audit profile of the study participants in a community based deaddiction camp. Methodology: A cross sectional survey was conducted at Suttur rural field practice area of JSS Medical College among the participants of a deaddiction camp organized by Alcoholics Anonymous and JSS Mahavidyapeetha in November 2014. All the participants were surveyed using AUDIT form for knowing the level of addiction and a pre tested questionnaire was used for collecting socio demographic information along with social factors influencing the alcohol use. Results: Majority, 76.4% have consumed alcohol more than 4 times a week and 23.6% have consumed alcohol 2 to 3 times per week. 96.4% of the study participants were alcohol dependents, 3.6% were in the zone of hazardous drinking and none were in the harmless AUDIT score zone. Majority of the participants, 43.6% were either injured or have injured someone else as a result of drinking. Conclusion: Most of the participants were alcohol dependents who will require specialist care and treatment in de addiction centers. Social Case Work, Social Group Work including Group therapy and family therapy could be initiated for the dependents. Introduction to the self support systems at home and in the community for the participants and the family members will help in reducing the alcohol dependency. Peer education and counseling will help the participants in adopting a healthy life styles and behaviours. Introduction Alcohol is the commonest substance abused by the human beings. According to WHO estimates, in 2012, about 3.3 million deaths, or 5.9% of all global deaths, were attributable to alcohol consumption. In 2012, 139 million DALYs (disability-adjusted life years), or 5.1% of the global burden of disease and injury, were attributable to alcohol consumption.1 The Global strategy to reduce the harmful use of alcohol defines “harmful use” as drinking that causes detrimental health and social consequences for the drinker, the people around the drinker and society at large, as well as the patterns of drinking that are associated with increased risk of adverse health outcomes.2 According to WHO estimates, there are about 2 billion people worldwide who consume alcoholic beverages and 76.3 million with diagnosable alcohol use disorders. The proportion of population in different groups of drinking spectrum varies considerably in different societies. WHO says alcohol is the major cause of death and disability in developing countries. India is the one of the largest producers of alcohol in the world and contributes to 65% of production and nearly 7% of imports into the South East Asian region.3 According to National Household Survey in India, the current prevalence of alcohol use among adult males is around 21%. It varies from as low as 7% in the western state of Gujarat to 75% in the north-eastern of Arunachal Pradesh. Significantly, higher use has been recorded among tribal, rural and lower socio-economic urban sections.4 The consumption of alcohol has been growing rapidly over the last two decades and alcoholic beverages are a standard lubricant at social gathering and those who refuse to consume run the risk of being social outcasts. Alcohol misuse is a general term for any level of risk ranging from hazardous drinking to alcohol dependence. Alcoholism and alcohol abuse are two different forms of problem drinking. Alcoholism occurs when a person shows signs of physical addiction to alcohol and continues to drink despite problems with physical and mental health .In alcohol abuse a person’s drinking leads to problems but not physical addiction. Among those who consume alcohol the spectrum of use range from one time use, regular use, hazardous use to harmful use. Hazardous use is the pattern of consumption carrying a risk of harmful consequences to the drinker may be physical or mental damage or social consequences to the drinker or others. Harmful use is the pattern of drinking that is causing damage to physical or mental health. Alcoholism leads to physical, psychological and socio-economic consequences. The AUDIT was developed by the World Health Organization (WHO) as a simple method of screening for excessive drinking and to assist in brief assessment. It can help in identifying excessive drinking as the cause of the presenting illness. It also provides a framework for intervention to help hazardous and harmful drinkers reduce or cease alcohol consumption and thereby avoid the harmful consequences of their drinking.5 Deaddiction and rehabilitation of alcoholics is a very crucial step to mainstream such demarginalised members of the society. The family and community at large play a very important role in reintegrating those with alcohol abuse. The community based camps provides easy access for those addicted to overcome their illness in a reassuring environment. The camp approach has been advocated as an effective alternative to hospital-based treatment of drug and alcohol dependence, offering many advantages such as direct participation of the community in the treatment process, better acceptance by the patients, better compliance and cost-effectiveness.6 Methodology: A community based alcohol de-addiction camp was conducted at Suttur Village, Nanjangud taluk, Mysuru District. The present community based cross-sectional study was conducted among the 55 participants who were attending this community based de-addiction camp. The participants were surveyed using AUDIT form specially prepared by World Health Organization (WHO) to assess and understand the level of addiction among alcoholics. A pre tested questionnaire was used for collecting socio demographic information along with social factors influencing the alcohol use. Written informed consent was taken from each of the participants. The questionnaire comprises of secondary variables such as gender, age, social status, demographic status and other psychosocial factors motivates the individuals to get addicted to it. Individual privacy and secrecy of gathered data was ensured before conducting the interview. Researcher has adopted purposive sampling method for the collection of data from the respondents. Gathered data was analyzed using SPSS (20.0) version. Qualitative data were expressed as proportions and quantitative data as mean with standard deviation. No association could be found statistically since variability in the group was uniform. Study Tool According to the WHO guidelines alcohol use disorders identification test, the individuals are classified based on their Audit scores under four zones. Those with a score of 0-7 fall within the harmless zone and need alcohol education, 8-15 within the hazardous drinking zone needs simple advice, 16-19 as those having severe alcohol problem needs simple advice plus brief counselling and continued monitoring and those with a score of 20-40 as alcohol dependents who require referral to specialist for diagnostic evaluation and treatment.7 Results There were 55 participants who attended the camp. All of them belonged to Hindu religion out of which 23.6 % were using alcohol 2 to 3 times a week (with 95 % CI 23.56,27.37 ) and rest were using alcohol more than four times a week. 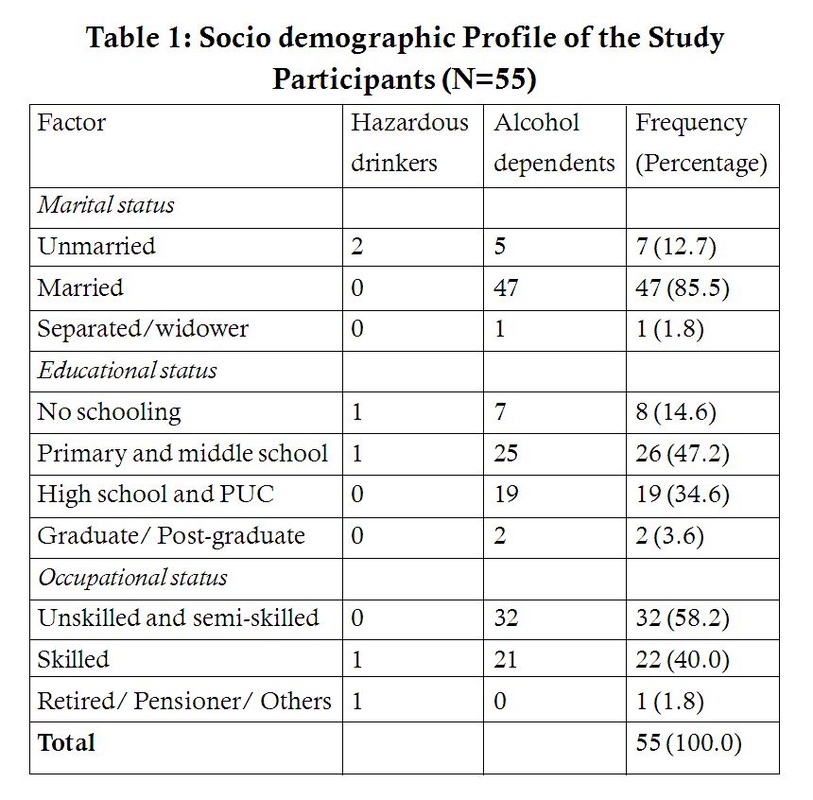 Majority, of the study participants (85.5%) were married, majority of them were educated (85.4%) and among them a half of them had studied at least up to primary school. Most of the study participants were unskilled or semi skilled worker (58.2%). 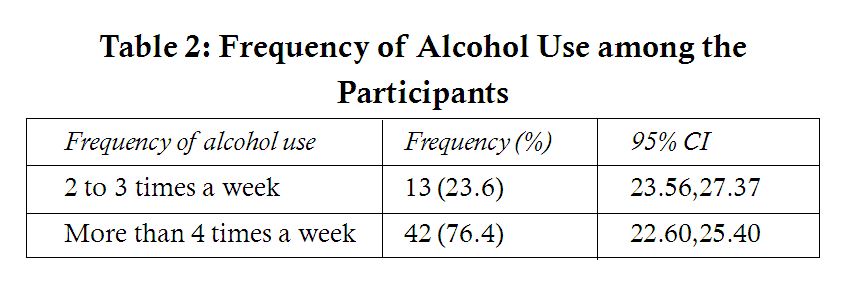 Majority, 76.4% have consumed alcohol more than 4 times a week and 23.6% have consumed alcohol 2 to 3 times per week. 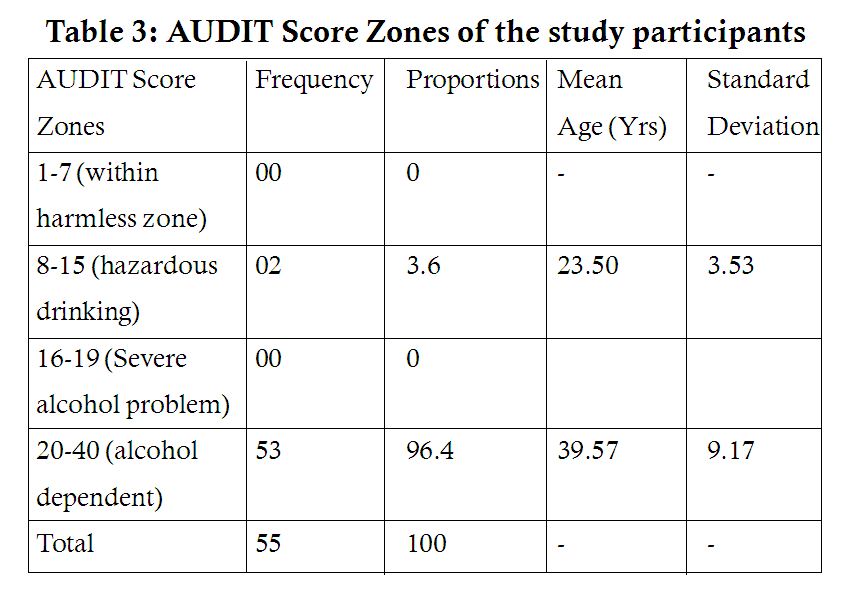 None of the study participants were within the harmless or severe alcohol problem zones of AUDIT score. 96.4% of the study participants were alcohol dependents, 3.6% were in the zone of hazardous drinking and none were in the harmless AUDIT score zone. The mean age was found to be 23.5 years among hazardous drinking, and 39.57 years among alcohol dependents indicating a higher AUDIT score among older persons. 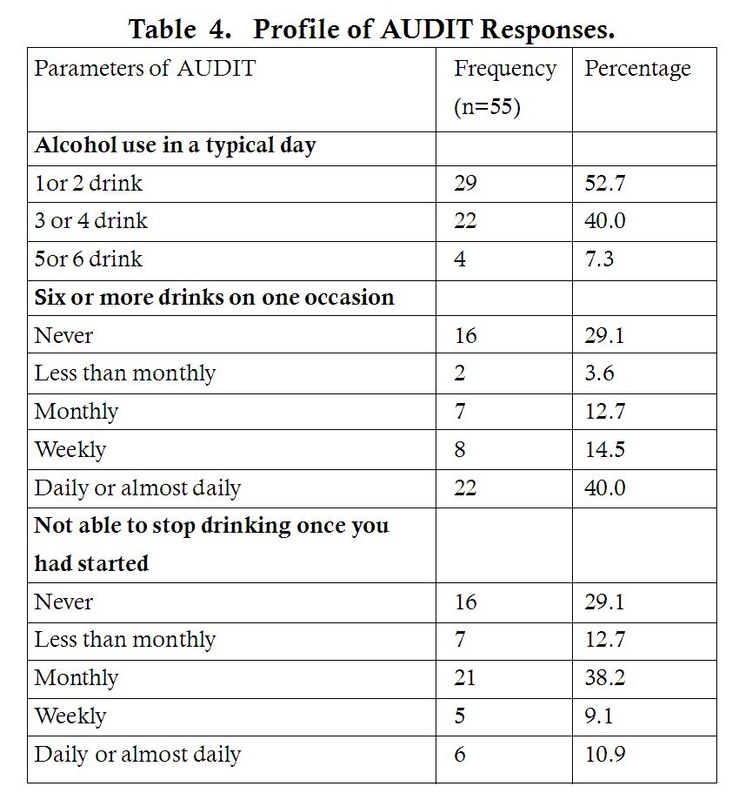 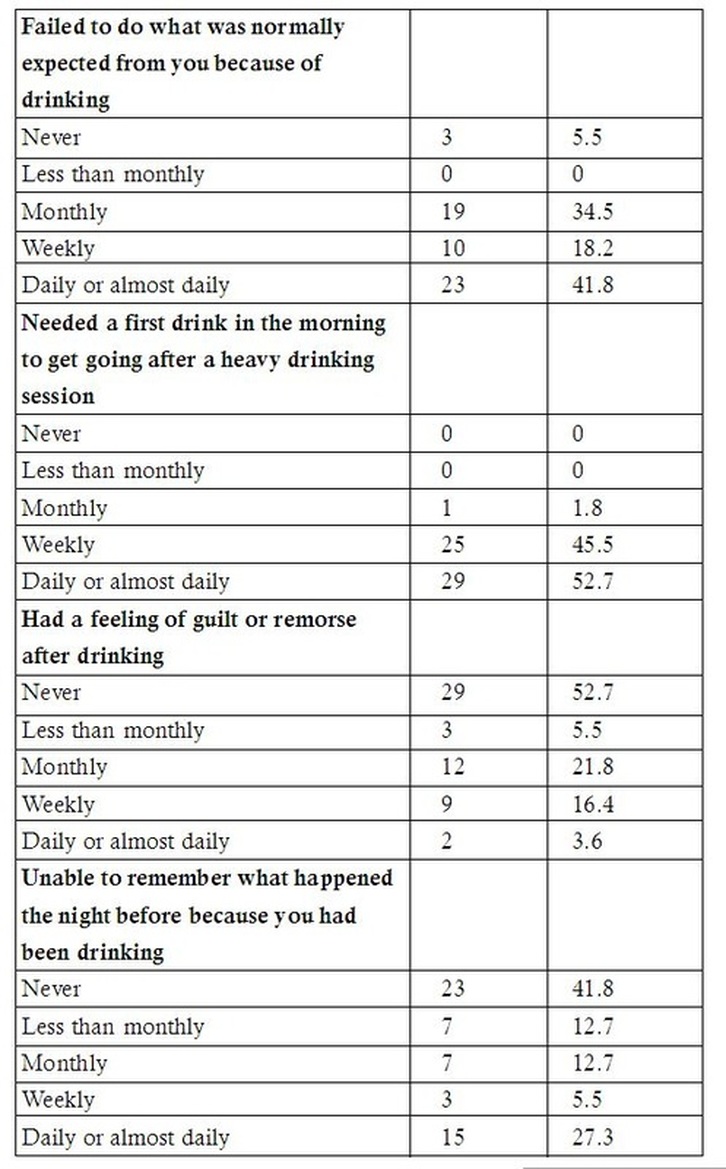  Most of them, 52.7% had consumed 1 or 2 drinks in a typical day.
Around 40% had consumed 6 or more drinks on one occasion daily or almost daily. Around 38% of the participants felt that they were unable to stop drinking once started monthly. Around 41% of the participants responded that daily or almost daily they failed to do what was normally expected from them because of drinking. Most, 97% responded that they needed a first drink in the morning to get going after a heavy drinking session either daily or weekly. Majority, 53% of the participants have never had a feeling of guilt or remorse after drinking. Around 48% of the respondents were unable to remember what happened the night before because of drinking. Majority of the participants, 43.6% were either injured or have injured someone else as a result of drinking. Around 78% of the respondents claimed that someone was concerned about their drinking or had been suggested to cut down. Discussion As described in table 1, most of the study participants (96.4%) were in alcohol dependent category according to AUDIT classification that had scores of more than 20 on the scale; this is expressed in other studies also since at this stage individual has reached problematic for the family as well as community. All of the participants belonged to Hindu religion which might be because of locality of the camp also the institution which conducted the programme of de-addiction belongs to same religion. This is explained by absence of religious customs abstaining from alcohol in Hindu religion. The mean and median age in years of the study participants was found to be 38.98 and 36 respectively. All the participants were males. Majority, of the study participants (85.5%) were married, majority of them were educated (85.4%) and among them a half of them had studied at least up to primary school. Most of the study participants were unskilled or semi skilled worker (58.2%). In a study by Umesh Tonse et al, the Mean age of the respondents in Community based de-addiction camp was 35 years and 40 years in Hospital based de-addiction camp respondents. Mean years of education in Community Based Camp was 5 years whereas in Hospital Based Camp it was 8 years. In the both groups, majority of the respondents were married (63%), 93% in Hospital Based Deaddiction Camp and 100% in Community Based Deaddiction Camp were Hindus. Majority of the respondents in the both the groups were employed, were semiskilled labourers.8 In a study by Shubh Mohan Singh et al majority of the participants (76.7 %) were married, most of them (70.4%) were literates and majority (78.0%) were skilled workers. The socio demographic profile of study participants in above studies was similar to our study population. The mean age of initiation of first consumption is 22.8 years which is higher than in a study by grant et al in which early initiation of alcohol use (before 14 years of age) is a predictor of impaired health status because it is associated with increased risk for alcohol dependence and abuse at later ages.9 As described in table 3, none of the study participants in this study were within the harmless or severe alcohol problem zones of AUDIT score. Majority were alcohol dependents requiring interventions as shown by higher AUDIT scores. The AUDIT scores were higher as age progresses which were evidenced as mean age among the participants suggesting that independence and early initiation could have contributed. As described in table 4, one in nine respondents needs a first drink in the morning which was a matter of due concern for the family members. One eighth of the participants had someone concerned about their alcoholic problem and was advised to attend a health facility for correction. All the participants have attended the correction facility only because of concern from one family member or another which shows a lack of voluntariness to attend facilities for correction on the part of respondents. A half of them was either injured or has injured someone else as a result of their drinking problem which might be detrimental and poses a serious in the social context. Strength – This study is conducted in rural community based setting rather than tertiary hospitals were de-addiction is usually done. Also it reduces self selection bias which is common in hospital based de-addiction camp. AUDIT is an internationally accepted and standardized tool. Limitations Sample size is limited to prove statistical significance. Inherent limitation of survey to elicit responses which includes some percent of recall and reporting bias. Conclusion Alcoholism is the major public health problem especially in rural India. Attention should be made to bring down the problems related to the alcohol menace. Most of the participants were alcohol dependents that will require specialist care and treatment in de addiction centers. The scoring pattern of AUDIT also highlights that only people with hazardous drinking or already dependent individuals having social problems are attending this de addiction camp. They are failed in primary as well as secondary screening of alcohol as per our AUDIT internationally accepted tool to assess the dependency of alcohol. Social Case Work, Social Group Work including Group therapy and family therapy could be initiated for the dependents. Introduction to the self support systems at home and in the community for the participants and the family members will help in reducing the alcohol dependency. Peer education and counseling will help the participants in adopting a healthy life styles and behaviours. Screening at all levels using the AUDIT scale helps in picking the people with the problem of drinking in turn helps in early diagnosis and treatment. Primordial level of prevention use in mass screening will help in reducing the burden of alcoholism apart from implementation of already existing law and policy. References
|
Categories
All

Social Work Learning Academy
50,000 HR PROFESSIONALS ARE CONNECTED THROUGH OUR NIRATHANKA HR GROUPS.
YOU CAN ALSO JOIN AND PARTICIPATE IN OUR GROUP DISCUSSIONS. 
MHR LEARNING ACADEMYGet it on Google Play store
|
 RSS Feed
RSS Feed
SITE MAP
SiteTRAININGJOB |
HR SERVICESOTHER SERVICESnIRATHANKA CITIZENS CONNECT |
NIRATHANKAPOSHOUR OTHER WEBSITESSubscribe |
MHR LEARNING ACADEMY




50,000 HR AND SOCIAL WORK PROFESSIONALS ARE CONNECTED THROUGH OUR NIRATHANKA HR GROUPS.
YOU CAN ALSO JOIN AND PARTICIPATE IN OUR GROUP DISCUSSIONS.
YOU CAN ALSO JOIN AND PARTICIPATE IN OUR GROUP DISCUSSIONS.


|
|